Check this out. So that you can giggle along. It’s good for lowering your stress level.
Health
What is gaslighting?
Gaslighting = trying to drive someone else crazy, literally. Because it makes you feel powerful. In control.
Watch this video. When he says that she is 30 minutes late for their first dinner, that’s when it starts. She was not late at all, but he wants her to start doubting herself. That’s gaslighting. Gaslighting also includes telling the people around you lies about you and getting them to abuse you too. Such people are called “flying monkeys”. It’s intended to help isolate the victim because that makes it possible to take the psychological abuse up a few notches. You can see that in this video as well.
Anyone who considers this kind of abuse hilarious should see a mental health professional. Because you may need to learn some techniques for how to modulate your behavior. That could be really helpful.
Dealing with the change in season
Yesterday, I talked about how I am dancing it out to music as a way to get in better shape again. Believe me, I need it.
Something else that I wanted to do something about concerns the changing seasons. It’s so much harder to get up when it’s still dark and my alarm often wakes me rather roughly. After I switch it off, I sometimes even fall asleep again whereas I was often up before 6am in the summer, without alarm.
What I used to do in the past is use a floor lamp on a timer to start waking me up. It’s much gentler and the light bulb I used for that is an energy-saving bulb that starts up slowly and spreads a warm glow. That likely makes it an older CFL (compact fluorescent light bulb). It certainly is pretty old.
So I went looking for a timer. I had two mechanical timers, one of which was broken (a spring in it seems to have snapped, but I am unable to open it), but I don’t like the noise that these mechanical timers make. I had a digital one too. Those are more complicated to program, but I managed.
The floor lamp that I want to use it with, in which I replaced the switch a long time ago with the aid of Wilko (because what it came with was rather clumsy), seemed to have developed a problem. Or maybe it is the bulb. Not sure yet. It started giving off a loud buzz, but only after a while (which makes it likely that the bulb is the problem).
Could also be that something was a little too loose in the lamp; it has a flexible “snake top” so it gets fiddled with.
So I took the lamp apart because it could do with a clean, did encounter a component that surprised me by falling out right away and that could have been the cause of the buzz (part of the bayonet fitting), gave it all a good clean and will do the final bit of reassembly later. I want the metal shade to dry well first. If in doubt, I will stop using this floor lamp, of course.
I will also test the bulb in that case, to make sure that it is not the source of the buzz after all. Bulbs can certainly buzz too and this bulb, like I said, is pretty old but still trucking. It could be telling me that it’s reached the end of its life or that, because it’s old, it’s not fully compatible with the newer digital timer.
What also helps a lot with getting up when the mornings are darker is… daylight bulbs! Get yourself a daylight bulb and switch that on after you’ve woken up. It helps kick-start your adrenaline serotonin cycle into adrenaline mode.

Dance it out, shake it off!
Lots of us, certainly women my age, so I understand, aren’t getting enough exercise these days.
Me, I started running when I was still in primary school and was blessed with a vast nature area behind our house.
If you’re in the middle of the urban environment, such as in Amsterdam, running outdoors often isn’t much fun. These days, I prefer grass and other natural surfaces to run on anyway. That’s gentler on tendons and joints and on your feet too.
So I increasingly often went on long walks.
In 2017, I had a one-sided viral pneumonia, however, and it took me a long time to bounce back from that in terms of energy level. Next, we had the pandemic with almost two years of pretty strict lockdowns.
The stretch that I used to walk is no longer available. I’d have to walk through traffic for about an hour, a lot of that traffic pretty heavy, causing the kind of non-stop noise that can leave you with a tension headache, to reach a nature reserve where I could walk around for a while, but then I’d have to walk back through traffic again for about an hour.
There is a lovely nearby cemetery where I can walk around and around and where I’ve also run in the past. But that’s not enough and becomes dull pretty quickly.
I found a distant but lovely stretch of grass that I can walk to and where I can then can walk around and around, but (the grass is often wet these days and) it’s more suitable for warmer weather, when you can saunter home and not feel that you “have” to walk to it and “have” to walk back from it.
So here’s an alternative, if you like music. It’s a playlist I started putting together during the pandemic lockdowns. More fun than an elliptical trainer and unlike exercise equipment, it takes up no precious space in your home, just speakers and you dancing it out, shaking it off.
Shake it off!
You can do this at any time (headphones on if needed) and for as long or briefly as you like.
It’ll really cheer you up!
PS
Logitech Z120 speakers are pretty decent.
Workplace PTSD

DEFRA consultation on regulation of genetic technologies (closes 17 March)
DEFRA currently has a consultation called “the regulation of genetic technologies”. Post-Brexit adaptations or not? Will we drop the phrase “even if their genetic change(s) could have been produced through traditional breeding” or not?
Post-Brexit, animal welfare protections are being abandoned. We can’t let that continue unbridled. This consultation is not just about animals, however. It is also about agriculture, bacteria and foodstuffs.
If you want to weigh in, you have up to 17 March, 1 minute before midnight. It will take you some time and you’d better have a bunch of references and links to data ready.
consult.defra.gov.uk/agri-food-chai
It consists of two parts, that is, the actual consultation is Part 1. You can come back to Part 2 later after you’ve completed Part 1. I have been working on Part 1 so far.
When I downloaded the 14-page document that goes with this gene editing consultation, I spotted several problems. There is a pretence of an emphasis on science and there is at least one or one half paragraph that has nothing to do with genetic technologies (obfuscation).
The document starts as follows:
“Building back greener is integral to creating a healthier, more resilient world for future generations and the Prime Minister has highlighted the need to take a more scientifically credible approach to regulation to help us meet some of the biggest challenges we face.”
This is the document’s fourth paragraph:
“While GE is unlikely to be able to address all these complex challenges, a whole range of innovative approaches could help us make progress over time. These could include increasing agro-ecological approaches for land management, the use of robotics and artificial intelligence, vertical farming, and the development of undervalued protein sources.“
The part in blue has nothing to do with gene editing. So why throw it in? The first sentence seems to suggest that there may not even be a need for gene editing. What is the purpose of this paragraph? To obfuscate?
On page 5 it says:
“Our position follows the science, which says that the safety of an organism is dependent on its characteristics and use rather than on how it was produced.”
That, with all due respect, sounds like pretentious nonsense. No references are given, no scientists are mentioned, no agencies or universities are named.
Anyone wishing to take part in this consultation, however, is supposed to provide evidence and literature references and the consultation is clearly not intended to draw the public’s opinion.
Also on page 5 of the consultation document, DEFRA mentions that Japan, Brazil, Australia and Argentina take a different position than the EU and there is the suggestion that the EU’s view is flawed.
“Now the transition period has ended, retained EU law requires that all GE organisms are classified as GMOs irrespective of whether they could be produced by traditional breeding methods. This was confirmed by a Court of Justice of the European Union (CJEU) judgment in 20181. This is not consistent with the position taken by most countries who have reviewed their respective regulations like Argentina, Australia, Brazil and Japan, which have concluded that certain GEOs should not be regulated as GMOs.”
There is also a 2-page Gene Editing Explainer, which tells the public what to think, again without providing any literature references or links.
(Only Rothamsted Research in Hertfordshire is mentioned in it. Wikipedia says:
“previously known as the Rothamsted Experimental Station and then the Institute of Arable Crops Research” “one of the oldest agricultural research institutions in the world, having been founded in 1843”. It is located on the campus of “Rothamsted Enterprises”. I assume that it is comparable to some of the departments of Wageningen University and Research. I am unfamiliar with it, had never heard of it before.)
I am a little disgusted with the approach taken by DEFRA here. I have taken part in DEFRA consultations before, when that particular PM mentioned at the start of the document was not PM yet. I may not often agree with DEFRA, but DEFRA’s consultations did not use to annoy me. This one does.
It is a political document, isn’t it?
I may be way off, but I hear the PM’s voice in the background and I sense the assumption that the public at large does not have the capability to understand the science and/or that the public is not well informed enough to be able to contribute to this consultation.
(Note that research in Germany showed that providing more information did not make the public more accepting of the use of genetic technologies; link below. These kinds of studies are not my field of expertise and there may be plenty of studies that found the opposite. But if that were the case, then why did DEFRA provide so little information?)
Below are my two cents, so far. Also biased, namely skewed toward caution, and written off the cuff.
In my opinion, organisms developed using genetic technologies such as gene editing (GE) must continue to be regulated as genetically modified organisms (GMOs) even if their genetic change(s) could have been produced through traditional breeding.
- Genetic technologies can have side effects that are not necessarily instantly clear. An example could be that the changes that Dr He introduced in a pair of human twins in China to make them immune to HIV could also have resulted in “off-target” changes and scientists are largely still in the dark about this. (Natural breeding does not have the potential for unintended changes that CRISPR still has.)
- The application of genetic technologies may also impact animal welfare differently than when their genetic change(s) are produced through traditional breeding.
Regarding the question as to the risk associated with the application, the problem is that we cannot predict what we don’t know yet.
If you look back into history, you can see that in the past, we’ve often hailed as great progress what we later ended up banning.
- We gave a Nobel Prize in medicine for the development of DDT. It almost eradicated the American bald eagle and that is only one aspect of its many side effects. DDT causes nerve damage and affects the hormone-producing systems of many animals, among other things lowering their fertility. In the United States, it was the environmentalist and marine biologist Rachel Carson’s work that eventually led to a ban on DDT and other pesticides.
- We didn’t even foresee the blatantly obvious consequences of insecticides, namely that their use would affect pollination as well as bird populations.
- Should I mention thalidomide? DES? That ibuprofen may affect male fertility?
- Many people are pushing to have other harmful pesticides banned, such as glyphosate and chlorpyrifos. That isn’t because they’re afraid of progress. It’s because these substances are not as harmless as we thought.
- When I was still based in the Netherlands and a board member of the Environmental Chemistry (and Toxicology) Section of the Royal Netherlands Chemical Society, our section organised a symposium on brominated flame retardants. They were already being found in tissues of animals in the Arctic. Did we see any of that coming? No, we did not. Subsequently, there was a push to phase them out in favour of others that turned out to have similar problems.
- Did we expect to do damage to the ozone layer when we introduced CFCs?
- Should I mention PFAS? (You may want to look into the situation in the Netherlands, where PFAS in soil have caused major upheaval because the Dutch want very little of it in their soils and the stuff is everywhere. When permitted levels were lowered, construction ground to a halt all over the country.) But we all thought that non-stick coatings (also called Teflon, PTFE, polytetrafluorethylene etc) were the greatest thing since sliced bread. People with pet birds started noticing disastrous effects. Perfluorooctanoic acid (PFAO), also known as C8, dissolves well in water and does not decay. It is now globally present in the air and in seawater. In the Netherlands, discharges by the Chemours plant in Dordrecht led to increased PFOA concentrations in the Merwede river and in the groundwater along its banks. In the U.S., a former DuPont plant in West Virginia released more than 1.7 million pounds of C8 into the region’s water, soil and air between 1951 and 2003. C8 was phased out after a class-action lawsuit that alleged that it causes cancer. Chemours now makes a new compound called GenX instead, for which safety thresholds have yet to be established. Regular water treatment methods don’t remove it from drinking water. GenX may be safer than C8, but it is also alleged to have caused tumours and reproductive problems in lab animals.
None of what I just wrote has anything to do with the use of genetic technologies. My point is that we never know with 100% certainty that all forms of progress are safe and we have missed the blatantly obvious in the past. This uncertainty also goes for genetic technologies.
I also think that dropping “even if their genetic change(s) could have been produced through traditional breeding” would likely make the regulation harder to apply. It would have companies trying to find all sorts of shortcuts (to “prove” that the effect of the technology they used could also have been produced through natural breeding). It might lead to frustrating discussions and costly legal proceedings. It might even lead to more campaigning, protests, etc.
(I did not look into how Japan, Brazil, Argentina and the United States handle these matters.)
There might well be effects on trade as well. German consumers for example traditionally have put great emphasis on ensuring that their food is as “clean” as possible.
https://www.loc.gov/law/help/restrictions-on-gmos/germany.php
https://www.researchgate.net/publication/326462738_Does_information_change_German_consumers’_attitudes_about_genetically_modified_food
From the abstract:
“The consumers who are more accepting of genetic modifications are younger, less educated and less concerned about their nutrition. The average effect of our provided information is negligible. However, the initially less opposed become slightly more opposed. Our results thus do not support the view that a lack of information drives consumer attitudes. Instead, attitudes seem to mostly reflect fundamental preferences.”
Many of the questions and the choices for answers in the DEFRA consultation survey are blatantly biased and it is quite clear that DEFRA would like to see the phrase “even if their genetic change(s) could have been produced through traditional breeding” dropped.
Am I being too critical? I don’t think so.
See also for example these two articles:
https://angelinasouren.com/2018/12/11/an-opinion/ by Cecile Janssens, professor at Emory University. A quote: “Most DNA mutations do nothing else other than cause the disease, but DNA variations may play a role in many diseases and traits. Take variations in the MC1R “red hair” gene, which not only increases the chance that your child will have red hair, but also increases their risk of skin cancer. Or variations in the OCA2 and HERC2 “eye color” genes that are also associated with the risk of various cancers, Parkinson’s and Alzheimer’s disease. To be sure, these are statistical associations, reported in the scientific literature, some may be confirmed; others may not. But the message is clear: Editing DNA variations for “desirable” traits may have adverse consequences, including many that scientists don’t know about yet.“
https://www.nature.com/articles/d41586-019-02087-5
So, what exactly is the science that DEFRA claims to be following? It is not this kind of science.
It is too soon to abandon caution.
12 March 2021
Here is the PDF with my response:
I expected Part 2 to take as long as Part 1 – I imagine that the start of Part 2 is the point at which many give up – but it did not. And in essence, it was a repeat of Part 1.
Homeless? You may soon no longer be breaking the law
Secretary of State for Housing, Communities and Local Government, Robert Jenrick MP, has told the House of Commons that the Vagrancy Act should be “consigned to history”.
Oh, that’s good of him, isn’t it?
At the same time, the UK government has quietly eroded the corona virus eviction protection – which was much less extensive than the one in the US to begin with – Lime Legal informed me this morning. It pointed me towards this article:
https://www.theguardian.com/society/2021/feb/28/eviction-orders-being-issued-despite-uk-government-covid-pledge
Excellent COVID-19 resource for decisionmakers at various levels
I started attending various webinars some time ago, like lots of people, and like lots of people, I also got a little webinar fatigue at times. ![]()
A great series continues to be organised by the National Academy of Medicine and the American Public Health Association in the US, looking into many topics such as the science of the virus, finding vaccines, health inequalities and so on.
Today’s session, on mitigating direct and indirect impacts in the coming months, was excellent for decisionmakers at all levels – also in the UK! – because it addressed a lot of practical aspects and many angles of the pandemic.
It mentioned the need to provide free wifi, talked about telehealth (telemedicine) and developments expected to take a decade suddenly being realised in a mere three weeks, about the complications food deserts pose, about the politicizing of the pandemic, about how to cope with emergencies such as hurricanes and related evacuations, how to remedy the impact the pandemic is having on non-Covid-related healthcare (such as people with heart attacks not seeking help out of fear of catching the virus), the healthcare clinics getting into financial difficulties as a result (as, I think, we saw earlier with those two doctors in California who owned a small chain of facilities and saw their turnover drop so dramatically that they resorted to unorthodox action), the challenge and need to communicate well and perhaps have ambassadors explain the purpose and reasoning behind social distancing, the massive impact social distancing has on the infection rate and the risk of people that people will no longer observe distancing when lockdowns are relaxed and developing a false sense of safety, and so on and so forth.
Here is a link for a model (simulator) that people can play with to explore the effects of lifting lockdowns: https://budgetmodel.wharton.upenn.edu/
The video recording of the webinar will be online soon, at covid19conversations.org:
https://covid19conversations.org/webinars/summer.
The slides have already been uploaded, but not all presenters used slides and the Q&A of course is not online yet either. I’ll post the unedited transcript below.

The corona virus crisis: My message to the police in the UK
In this video, I ask British police to be understanding toward us when enforcing the social distancing rules because, in spite of the fact that the lock-down resembles being imprisoned to some degree, we haven’t actually done anything wrong.
Police officers should also comply with the rules themselves.
And we have a posterboy !
 Boris Johnson is in hospital (and to my surprise, I managed to tweet the news before most of the UK news sites posted it because a financial news popup on my screen beat them to it).
Boris Johnson is in hospital (and to my surprise, I managed to tweet the news before most of the UK news sites posted it because a financial news popup on my screen beat them to it).
I wish him and his pregnant partner well. Of course I do!
The good news?
He may now become the posterboy for making people take this thing seriously and stop assuming that only “dumb people in other countries” and “old folks” get knocked down by it.
This is no time for cavalier attitudes, unless it is the kind of attitude that Captain Crozier displayed. He is the kind of hero we need now.
And the kind of heroes who work and volunteer on the front lines of all care as well as the people who continue to deliver postal mail, who are at work at the supermarkets, supply them with stock and all the others who continue to keep as many things working as possible.
Landlords…
Never had any problems with landlords in the Netherlands. Never.
Had three in Florida. The first and the third were fine, but the second one was not and his attorney was rumoured to have mafia ties, I kid you not. But I heard that later. I think it was actually a legal aid lawyer who told me that who I talked with later, long after I’d moved out and his lawyer started pestering me. I’ll spare you the details.
My third landlord was the husband of the person I volunteered with on Saturdays and sometimes Sundays. (He was a builder, built huge places, the way they are in Florida. Nice guy. I think he was in the US Army for a while, and they lived in places like Morocco. ) She stopped by one day – to bring me two birds – and was appalled and suggested I move in to one of their places. They owned a small apartment building that was mostly used by snowbirds (people from for example Canada who take winter vacations in Florida).
Some time later, I moved to Britain.
In Southampton, I knew several landlords. (Only one of them was mine.)
One said that only educated people were decent human beings, and I was too shocked to respond. He called tenants who rang him because the washing machine or heating wasn’t working (properly) “bad tenants”. This was not my own landlord, but someone I met within a business context and was friendly with for a while. Wasn’t actually a bad guy at all, strangely enough.
I also knew one who proudly told me how he had tricked an elderly woman with beginning Alzheimer’s out of her flat, I kid you not.
On another occasion, the same guy was talking with me about a new building he was constructing and then added that it did not have to be very good “as it is only for tenants”.
In Portsmouth, I’ve met two who dump rubbish on other people’s front courts and patios. I caught one red-handed and the other one admitted it.
I have principles.
If I can help make things better for people who come after me who are less strong in some way – okay, except physically as I am getting old and I am feeling it – I will try to do that. And that baffles the hell out of (most) Brits. But that is not my problem.
We need a global guideline for eugenics – urgently
People are currently focusing on Trump and his silly comments, but perhaps they should be focussing on Britain.
A few days ago, British newspaper The Guardian reported about a eugenics meeting that allegedly had been convened in secret, involving someone who has previously advocated child rape. This meeting is supposed to have taken place at University College London and white supremacists supposedly were present at this meeting. Continue reading
Tony Blair on social engineering
Interview with Mark Easton, BBC. Date unknown, but near the end of Tony Blair’s premiership.
Keep in mind that “hooliganism” and “anti-social behaviour” are often labels used to indicate (and reject) people from a lower socioeconomic class in Britain and that this “hooliganism” for example gets expressed in graffiti.
Of course, causing (increased) financial hardship for parents by taking any benefits away is most definitely not “in the best interest of the child”.
Tony Blair did consider graffiti “anti-social behaviour”. During a photo-op as part of his crusade, he hosed down graffiti and said that older generations of his family would have abhorred such behaviour. It then turned out that his own grandmother had been a “commie” graffiti vandal.
There probably is a work by Banksy somewhere in response to all of this.
Tony Blair also criminalized a lot of behavior that is essentially merely human behavior. That too was in nobody’s best interest and probably did nothing toward decreasing inequality in Britain.
It did not enable (more) people to flourish.
How seeing problems in the brain makes stigma disappear
Brain Imaging Research Division, Wayne State University School of Medicine, CC BY-SA
David Rosenberg, Wayne State University
As a psychiatrist, I find that one of the hardest parts of my job is telling parents and their children that they are not to blame for their illness.
Children with emotional and behavioral problems continue to suffer considerable stigma. Many in the medical community refer to them as “diagnostic and therapeutic orphans.” Unfortunately, for many, access to high-quality mental health care remains elusive.
An accurate diagnosis is the best way to tell whether or not someone will respond well to treatment, though that can be far more complicated than it sounds.
I have written three textbooks about using medication in children and adolescents with emotional and behavioral problems. I know that this is never a decision to take lightly.
But there’s reason for hope. While not medically able to diagnose any psychiatric condition, dramatic advances in brain imaging, genetics and other technologies are helping us objectively identify mental illness.
Knowing the signs of sadness
All of us experience occasional sadness and anxiety, but persistent problems may be a sign of a deeper issue. Ongoing issues with sleeping, eating, weight, school and pathologic self-doubt may be signs of depression, anxiety or obsessive-compulsive disorder.
Separating out normal behavior from problematic behavior can be challenging. Emotional and behavior problems can also vary with age. For example, depression in pre-adolescent children occurs equally in boys and girls. During adolescence, however, depression rates increase much more dramatically in girls than in boys.
It can be very hard for people to accept that they – or their family member – are not to blame for their mental illness. That’s partly because there are no current objective markers of psychiatric illness, making it difficult to pin down. Imagine diagnosing and treating cancer based on history alone. Inconceivable! But that is exactly what mental health professionals do every day. This can make it harder for parents and their children to accept that they don’t have control over the situation.
Fortunately, there are now excellent online tools that can help parents and their children screen for common mental health issues such as depression, anxiety, panic disorder and more.
Most important of all is making sure your child is assessed by a licensed mental health professional experienced in diagnosing and treating children. This is particularly important when medications that affect the child’s brain are being considered.
Seeing the problem
Thanks to recent developments in genetics, neuroimaging and the science of mental health, it’s becoming easier to characterize patients. New technologies may also make it easier to predict who is more likely to respond to a particular treatment or experience side effects from medication.
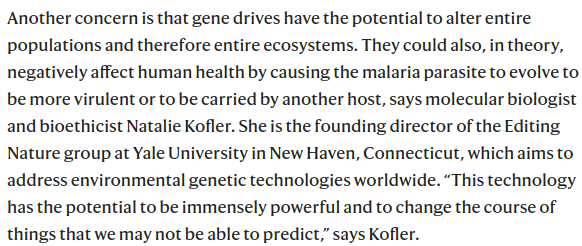
Our laboratory has used brain MRI studies to help unlock the underlying anatomy, chemistry and physiology underlying OCD. This repetitive, ritualistic illness – while sometimes used among laypeople to describe someone who is uptight – is actually a serious and often devastating behavioral illness that can paralyze children and their families.
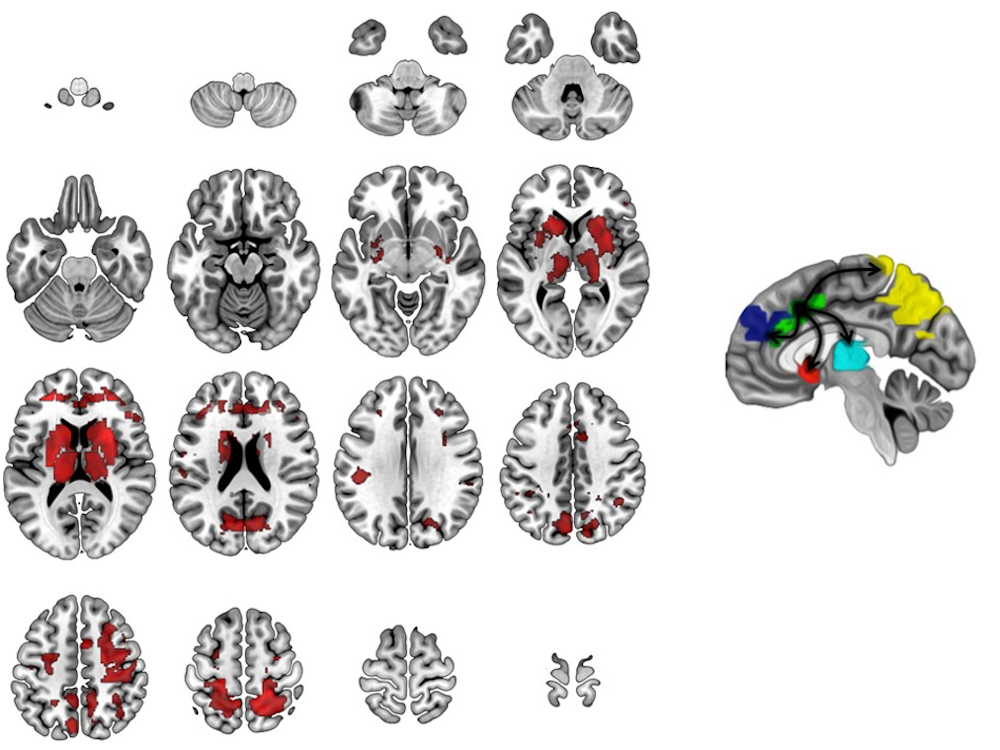
Image adapted from Diwadkar VA, Burgess A, Hong E, Rix C, Arnold PD, Hanna GL, Rosenberg DR. Dysfunctional activation and brain network profiles in youth with Obsessive-Compulsive Disorder: A focus on the dorsal anterior cingulate during working memory. Frontiers in Human Neuroscience. 2015; 9: 1-11., CC BY-SA
Through sophisticated, high-field brain imaging techniques – such as fMRI and magnetic resonance spectroscopy – that have become available recently, we can actually measure the child brain to see malfunctioning areas.
We have found, for example, that children 8 to 19 years old with OCD never get the “all clear signal” from a part of the brain called the anterior cingulate cortex. This signal is essential to feeling safe and secure. That’s why, for example, people with OCD may continue checking that the door is locked or repeatedly wash their hands. They have striking brain abnormalities that appear to normalize with effective treatment.
We have also begun a pilot study with a pair of identical twins. One has OCD and the other does not. We found brain abnormalities in the affected twin, but not in the unaffected twin. Further study is clearly warranted, but the results fit the pattern we have found in larger studies of children with OCD before and after treatment as compared to children without OCD.
Exciting brain MRI and genetic findings are also being reported in childhood depression, non-OCD anxiety, bipolar disorder, ADHD and schizophrenia, among others.
Meanwhile, the field of psychiatry continues to grow. For example, new techniques may soon be able to identify children at increased genetic risk for psychiatric illnesses such as bipolar disorder and schizophrenia.
New, more sophisticated brain imaging and genetics technology actually allows doctors and scientists to see what is going on in a child’s brain and genes. For example, by using MRI, our laboratory discovered that the brain chemical glutamate, which serves as the brain’s “light switch,” plays a critical role in childhood OCD.
What a scan means
When I show families their child’s MRI brain scans, they often tell me they are relieved and reassured to “be able to see it.”
Children with mental illness continue to face enormous stigma. Often when they are hospitalized, families are frightened that others may find out. They may hesitate to let schools, employers or coaches know about a child’s mental illness. They often fear that other parents will not want to let their children spend too much time with a child who has been labeled mentally ill. Terms like “psycho” or “going mental” remain part of our everyday language.
The example I like to give is epilepsy. Epilepsy once had all the stigma that mental illness today has. In the Middle Ages, one was considered to be possessed by the devil. Then, more advanced thinking said that people with epilepsy were crazy. Who else would shake all over their body or urinate and defecate on themselves but a crazy person? Many patients with epilepsy were locked in lunatic asylums.
Then in 1924, psychiatrist Hans Berger discovered something called the electroencephalogram (EEG). This showed that epilepsy was caused by electrical abnormalities in the brain. The specific location of these abnormalities dictated not only the diagnosis but the appropriate treatment.
![]() That is the goal of modern biological psychiatry: to unlock the mysteries of the brain’s chemistry, physiology and structure. This can help better diagnose and precisely treat childhood onset mental illness. Knowledge heals, informs and defeats ignorance and stigma every time.
That is the goal of modern biological psychiatry: to unlock the mysteries of the brain’s chemistry, physiology and structure. This can help better diagnose and precisely treat childhood onset mental illness. Knowledge heals, informs and defeats ignorance and stigma every time.
David Rosenberg, Professor, Psychiatry and Neuroscience, Wayne State University
This article was originally published on The Conversation. Read the original article.
The murky issue of whether the public supports assisted dying
Katherine Sleeman, King’s College London
The High Court has rejected a judicial review challenging the current law which prohibits assisted dying in the UK. Noel Conway, a 67-year-old retired lecturer who was diagnosed with Motor Neurone Disease in 2014, was fighting for the right to have medical assistance to bring about his death. Commenting after the judgement on October 5, his solicitor indicated that permission will now be sought to take the case to the appeal courts.
Campaigners are often quick to highlight the strength of public support in favour of assisted dying, arguing that the current law is undemocratic. But there are reasons to question the results of polls on this sensitive and emotional issue.
There have been numerous surveys and opinion polls on public attitudes towards assisted dying in recent years. The British Social Attitudes (BSA) Survey, which has asked this question sequentially since the 1980s, has shown slowly increasing public support. Asked: “Suppose a person has a painful incurable disease. Do you think that doctors should be allowed by law to end the patient’s life, if the patient requests it?” in 1984, 75% of people surveyed agreed. By 1989, 79% of people agreed with the statement, and in 1994 it had gone up to 82%.
Detail of the question matters
But not surprisingly, the acceptability of assisted dying varies according to the precise context. The 2005 BSA survey asked in more depth about attitudes towards assisted dying and end of life care. While 80% of respondents agreed with the original question, support fell to 45% for assisted dying for illnesses that were incurable and painful but not terminal.
A 2010 ComRes-BBC survey also found that the incurable nature of illness was critical. In this survey, while 74% of respondents supported assisted suicide if an illness was terminal, this fell to 45% if it was not.

from http://www.shutterstock.com
It may not be surprising that support varies considerably according to the nature of the condition described, but it is important. First, because the neat tick boxes on polls belie the messy reality of determining prognosis for an individual patient. Second, because of the potential for drift in who might be eligible once assisted dying is legalised. This has happened in countries such as Belgium which became the first country to authorise euthanasia for children in 2014, and more recently in Canada where within months of the 2016 legalisation of medical assistance in dying, the possibility of extending the law to those with purely psychological suffering was announced.
It’s not just diagnosis or even prognosis that influences opinion. In the US, Gallup surveys carried out since the 1990s have shown that support for assisted dying hinges on the precise terminology used to describe it. In its 2013 poll, 70% of respondents supported “end the patient’s life by some painless means” whereas only 51% supported “assisting the patient to commit suicide”. This gap shrank considerably in 2015 – possibly as a result of the Brittany Maynard case. Maynard, a high-profile advocate of assisted dying who had terminal cancer, moved from California to Oregon to take advantage of the Oregon Death with Dignity law in 2014.
Even so, campaigning organisations for assisted dying tend to avoid the word “suicide”. Language is emotive, but if we want to truly gauge public opinion, we need to understand this issue, not gloss over it.
Information changes minds
Support for assisted dying is crucially known to drop-off simply when key information is provided. Back in the UK, a ComRes/CARE poll in 2014 showed 73% of people surveyed agreed with legalisation of a bill which enables: “Mentally competent adults in the UK who are terminally ill, and who have declared a clear and settled intention to end their own life, to be provided with assistance to commit suicide by self-administering lethal drugs.” But 42% of these same people subsequently changed their mind when some of the empirical arguments against assisted dying were highlighted to them – such as the risk of people feeling pressured to end their lives so as not to be a burden on loved ones.
This is not just a theoretical phenomenon. In 2012, a question over legalising assisted dying was put on the ballot paper in Massachusetts, one of the most liberal US states. Support for legalisation fell in the weeks prior to vote, as arguments against legalisation were aired, and complexities became apparent. In the end, the Massachusetts proposition was defeated by 51% to 49%. Public opinion polls, in the absence of public debate, may gather responses that are reflexive rather than informed.
![]() Polls are powerful tools for democratic change. While opinion polls do show the majority of people support legalisation of assisted dying, the same polls also show that the issue is far from clear. It is murky, and depends on the responder’s awareness of the complexities of assisted dying, the context of the question asked, and its precise language. If we can conclude anything from these polls, it is not the proportion of people who do or don’t support legislation, but how easily people can change their views.
Polls are powerful tools for democratic change. While opinion polls do show the majority of people support legalisation of assisted dying, the same polls also show that the issue is far from clear. It is murky, and depends on the responder’s awareness of the complexities of assisted dying, the context of the question asked, and its precise language. If we can conclude anything from these polls, it is not the proportion of people who do or don’t support legislation, but how easily people can change their views.
Katherine Sleeman, NIHR Clinician Scientist and Honorary Consultant in Palliative Medicine, King’s College London
This article was originally published on The Conversation. Read the original article.
The science behind… coffee!
Brewing a great cup of coffee depends on chemistry and physics

Chris Hendon, CC BY-ND
Christopher H. Hendon, University of Oregon
Coffee is unique among artisanal beverages in that the brewer plays a significant role in its quality at the point of consumption. In contrast, drinkers buy draft beer and wine as finished products; their only consumer-controlled variable is the temperature at which you drink them.
Why is it that coffee produced by a barista at a cafe always tastes different than the same beans brewed at home?
It may be down to their years of training, but more likely it’s their ability to harness the principles of chemistry and physics. I am a materials chemist by day, and many of the physical considerations I apply to other solids apply here. The variables of temperature, water chemistry, particle size distribution, ratio of water to coffee, time and, perhaps most importantly, the quality of the green coffee all play crucial roles in producing a tasty cup. It’s how we control these variables that allows for that cup to be reproducible.
How strong a cup of joe?
Besides the psychological and environmental contributions to why a barista-prepared cup of coffee tastes so good in the cafe, we need to consider the brew method itself.

Chris Hendon, CC BY-ND
We humans seem to like drinks that contain coffee constituents (organic acids, Maillard products, esters and heterocycles, to name a few) at 1.2 to 1.5 percent by mass (as in filter coffee), and also favor drinks containing 8 to 10 percent by mass (as in espresso). Concentrations outside of these ranges are challenging to execute. There are a limited number of technologies that achieve 8 to 10 percent concentrations, the espresso machine being the most familiar.
There are many ways, though, to achieve a drink containing 1.2 to 1.5 percent coffee. A pour-over, Turkish, Arabic, Aeropress, French press, siphon or batch brew (that is, regular drip) apparatus – each produces coffee that tastes good around these concentrations. These brew methods also boast an advantage over their espresso counterpart: They are cheap. An espresso machine can produce a beverage of this concentration: the Americano, which is just an espresso shot diluted with water to the concentration of filter coffee.
All of these methods result in roughly the same amount of coffee in the cup. So why can they taste so different?
When coffee meets water
There are two families of brewing device within the low-concentration methods – those that fully immerse the coffee in the brew water and those that flow the water through the coffee bed.
From a physical perspective, the major difference is that the temperature of the coffee particulates is higher in the full immersion system. The slowest part of coffee extraction is not the rate at which compounds dissolve from the particulate surface. Rather, it’s the speed at which coffee flavor moves through the solid particle to the water-coffee interface, and this speed is increased with temperature.

Specialty Coffee Association of America, CC BY-NC-ND
A higher particulate temperature means that more of the tasty compounds trapped within the coffee particulates will be extracted. But higher temperature also lets more of the unwanted compounds dissolve in the water, too. The Specialty Coffee Association presents a flavor wheel to help us talk about these flavors – from green/vegetative or papery/musty through to brown sugar or dried fruit.
Pour-overs and other flow-through systems are more complex. Unlike full immersion methods where time is controlled, flow-through brew times depend on the grind size since the grounds control the flow rate.
The water-to-coffee ratio matters, too, in the brew time. Simply grinding more fine to increase extraction invariably changes the brew time, as the water seeps more slowly through finer grounds. One can increase the water-to-coffee ratio by using less coffee, but as the mass of coffee is reduced, the brew time also decreases. Optimization of filter coffee brewing is hence multidimensional and more tricky than full immersion methods.

Redd Angelo on Unsplash, CC BY
Other variables to try to control
Even if you can optimize your brew method and apparatus to precisely mimic your favorite barista, there is still a near-certain chance that your home brew will taste different from the cafe’s. There are three subtleties that have tremendous impact on the coffee quality: water chemistry, particle size distribution produced by the grinder and coffee freshness.
First, water chemistry: Given coffee is an acidic beverage, the acidity of your brew water can have a big effect. Brew water containing low levels of both calcium ions and bicarbonate (HCO₃⁻) – that is, soft water – will result in a highly acidic cup, sometimes described as sour. Brew water containing high levels of HCO₃⁻ – typically, hard water – will produce a chalky cup, as the bicarbonate has neutralized most of the flavorsome acids in the coffee.
Ideally we want to brew coffee with water containing chemistry somewhere in the middle. But there’s a good chance you don’t know the bicarbonate concentration in your own tap water, and a small change makes a big difference. To taste the impact, try brewing coffee with Evian – one of the highest bicarbonate concentration bottled waters, at 360 mg/L.
The particle size distribution your grinder produces is critical, too.
Every coffee enthusiast will rightly tell you that blade grinders are disfavored because they produce a seemingly random particle size distribution; there can be both powder and essentially whole coffee beans coexisting. The alternative, a burr grinder, features two pieces of metal with teeth that cut the coffee into progressively smaller pieces. They allow ground particulates through an aperture only once they are small enough.

Aaron Itzerott on Unsplash, CC BY
There is contention over how to optimize grind settings when using a burr grinder, though. One school of thought supports grinding the coffee as fine as possible to maximize the surface area, which lets you extract the most delicious flavors in higher concentrations. The rival school advocates grinding as coarse as possible to minimize the production of fine particles that impart negative flavors. Perhaps the most useful advice here is to determine what you like best based on your taste preference.
Finally, the freshness of the coffee itself is crucial. Roasted coffee contains a significant amount of CO₂ and other volatiles trapped within the solid coffee matrix: Over time these gaseous organic molecules will escape the bean. Fewer volatiles means a less flavorful cup of coffee. Most cafes will not serve coffee more than four weeks out from the roast date, emphasizing the importance of using freshly roasted beans.
One can mitigate the rate of staling by cooling the coffee (as described by the Arrhenius equation). While you shouldn’t chill your coffee in an open vessel (unless you want fish finger brews), storing coffee in an airtight container in the freezer will significantly prolong freshness.
![]() So don’t feel bad that your carefully brewed cup of coffee at home never stacks up to what you buy at the café. There are a lot of variables – scientific and otherwise – that must be wrangled to produce a single superlative cup. Take comfort that most of these variables are not optimized by some mathematical algorithm, but rather by somebody’s tongue. What’s most important is that your coffee tastes good to you… brew after brew.
So don’t feel bad that your carefully brewed cup of coffee at home never stacks up to what you buy at the café. There are a lot of variables – scientific and otherwise – that must be wrangled to produce a single superlative cup. Take comfort that most of these variables are not optimized by some mathematical algorithm, but rather by somebody’s tongue. What’s most important is that your coffee tastes good to you… brew after brew.
Christopher H. Hendon, Assistant Professor of Computational Materials and Chemistry, University of Oregon
This article was originally published on The Conversation. Read the original article.
Tasering of patients
Dutch daily Trouw prominently featured anger about a human rights violation on its 6 September front page (online version; 8 January 2010: this has been updated since I read the article and wrote this post).
 Not only had Dutch police tasered a patient in so-called drive-stun mode (“pain compliance“), the patient in question already was in solitary confinement.
Not only had Dutch police tasered a patient in so-called drive-stun mode (“pain compliance“), the patient in question already was in solitary confinement.
I was shocked when I read this. It seems to signal a return to practices I thought we had left behind a long time ago, and it particularly worries me that this happened in the Netherlands of all places.
“This is torture,” say Amnesty International as well as organizations of patients and their relatives, and Amnesty has called for an immediate suspension of the use of this type of weapon by Dutch police, so I understand. According to Trouw, the taser’s manufacturer advises against use on psychiatric patients and Amnesty believes taser use may actually be life-threatening in such cases.
This is likely the first time a taser was used to subdue a hospitalized psychiatric patient in the Netherlands, where three-hundred police officers are currently testing tasers.
The following appears to have transpired.
On 17 July, police officers were called to a hospital in Cappelle aan de IJssel, in which a male patient in his twenties was having a psychotic episode. (When Dutch police are called to a hospital for a problem with a patient, police take over responsibility.)
The patient was having a bad day, apparently, and had refused to take his antipsychotic medicines. Rotterdam police were first called to force the patient into solitary confinement (to reduce sensory input and calm the patient down).
In the evening, police were called again, for unknown reasons. That’s when the tasering occurred.
The patient’s mother, Marijke Bos, found out about the incident a few days later during a visit on her son’s birthday. Her son had dark bruises under his eyes, several bruises on one of his hips and roughly thirty small taser-related lesions on his back. The patient had also been tasered on one of his feet.
The patient’s mother has filed several formal complaints.
The hospital staff reportedly is also extremely dismayed about the taser use.
Solitary confinement in itself can be damaging and can be seen as a human rights violation. Tasering a patient who already is in solitary confinement and clearly no danger to anyone else raises eyebrows, to put it mildly.
It seems to me that tasering in drive-stun mode is even worse than using a baseball bat to knock someone out as it deliberately causes pain, so it is more comparable to stabbing someone with a knife or throwing scalding water or oil.
The incident made me wonder about taser use on patients in other countries and I did a quick web search. It is not clear whether other reports of taser use on patients concern drive-stun mode or probe mode, but probe mode is the usual taser mode.
New Zealand police used a taser on a mentally ill man earlier this year as well and it was the country’s second case this year in which taser use against a mentally ill person was ruled (excessive and) unjustified:
“Police told the 21-year-old he would need to be strip searched, the man repeatedly refused to remove his clothes telling the officers he had a history of sexual abuse and didn’t feel comfortable being touched by males.”
In Britain, even taser use in general has turned out to concern mainly mentally ill persons, according to Home Office figures:
Taser use against patients in hospitals has already around in Britain for more than ten years:
The consensus appears to be that this is a big no-no:
- http://thejusticegap.com/2016/12/must-ban-tasers-mental-health-system/
- http://www.iimhl.com/files/docs/Make_It_So/20161020.pdf
I agree with Matilda MacAttram (director of Black Mental Health UK and writer of the above article in the Guardian) that there is no role for police in mental healthcare, just like police have no business in heart surgeries and appendectomies either.
See also this article:
Will future parents need a license?
I ran into a discussion on Kialo, to which I quickly contributed the first paragraph below and penned what I have added below, all within about five minutes. I later edited it a bit, to make it easier to read.
 I am so pleased someone started this discussion. I promote non-discrimination of embryos and fetuses. A child is not a consumer product but a human being who must be loved and encouraged to flourish. How can you love one child but not another if the latter is non-mainstream? I’ve been thinking about that and it’s made me wonder if it actually means that the parents aren’t fit to be parents. I haven’t dared say that out loud yet, but this discussion clears the road for me.
I am so pleased someone started this discussion. I promote non-discrimination of embryos and fetuses. A child is not a consumer product but a human being who must be loved and encouraged to flourish. How can you love one child but not another if the latter is non-mainstream? I’ve been thinking about that and it’s made me wonder if it actually means that the parents aren’t fit to be parents. I haven’t dared say that out loud yet, but this discussion clears the road for me.
So yes, maybe parents-to-be should require vetting.
Within a few decades, we will no longer require sex to create babies, but will make our offspring in the lab, possibly on the basis of skin cells from each of the parents. We’ll probably look after our little gestating (incubating) children as if they are rare orchids that we want to bring to bloom.
(So by that time, women will no longer have a need for abortions and they won’t have to menstruate and experience PMS any longer either.)
I can imagine very well that you will require a license in the future in order to have a child. Somehow, that feels like an automatic consequence of the possibilities we will have then.
And also, indeed, why should adoptive parents be scrutinized but are natural parents free to do whatever they want?
And after all, in that distant future, anyone who wants can probably have a child (technically speaking). Even adoption may slowly become a thing of the past, that is, if we get to the point that we no longer succumb to illnesses and accidents and maybe even can choose when our lives end.
I hasten to add that at the moment, natural parents are not always free to do as they please either, of course. For example, in countries with a great deal of inequality, the state may step in on the basis of what is no more than prejudice in practice.
Nowadays, some children suffer horribly, either because of their parents or because of someone else. Sometimes before children are removed from their parents and sometimes afterward.
In practice, perhaps it won’t be an actual license but a training program that must be completed with good results. If that training is tough and long enough, that alone will already sort committed parents from parents who aren’t ready for a child.
Would they have to get a license or go through some kind of training program every time they want to have a child? Yes, I think so. Insights change.
It’s even possible that parenting will eventually become a profession.
PS
Unfortunately, Kialo may not work very well with Linux. I was able to post my contribution, but seem unable to comment on other people’s contributions. Maybe it’s part of the learning curve, but I did see the intro video and the comment option mentioned in it simply does not seem to exist for me.
My response to Dr Seidel’s post on the BMJ blog (Baby genome screening—paving the way to genetic discrimination?)
I just submitted the following comment, here:
http://blogs.bmj.com/bmj/2017/07/05/markus-g-seidel-baby-genome-screening-paving-the-way-to-genetic-discrimination/
It is still in moderation. has been accepted. Yes, it was far from flawless – I wrote most of it at the spur of the moment – but I think that what I mean is clear enough. I have done some editing in the version below.
Dear Dr Seidel, thank you for making these very important points.
I am taking the opportunity to offer a few suggestions for discussion and invite more views on these issues. Some of what I write below only emerged during the writing of this response and may not be watertight. Can you withhold initial judgement, think along with me and see it as an exercise in exploring the various angles?
But first of all, please forgive me my shortcomings; I phrase various concepts differently than you do as my background is not in medicine and I tend to shy away from jargon. Also, what I say is not limited to newborns, but that will be obvious to this audience. The principles largely remain the same, whether we are talking about a pre-embryo, a fetus or a newborn, and whether I call them person, individual or child. (Legally, this is currently much more complex, as you know.) My focus in this discussion does not extend to persons beyond the age of majority (likely not even beyond 8 or 10, in practice) and I am also keeping the concept of euthanasia out of the discussion even though it is related. Worst of all, I throw all techniques related to genetic material into one big pot because it enables me to see the bigger picture better.
I write from my own perspective of an opinionated white woman in the west, but when I say “we”, my intention is to refer to the human species. People from other cultures will undoubtedly spot biases in my western views; I would like those people to point out those biases.
You ask whether genome screening for newborns will pave the way to genetic discrimination. You also raise the question of the interpretation (and reliability) of such data and you have privacy concerns.
With regard to the latter, I think that we will slowly have to accept that the digital age comes with the loss of privacy in many ways. That does not have to be as dramatic as it sounds. Privacy is a changing concept anyway, which also has a cultural angle to it. The realization that people from different generations and from different cultures have slightly different views on what privacy is may add some perspective that can make us breathe easier. So we should probably become more relaxed about the loss of privacy as we knew it and focus more on preventing and ameliorating potential negative consequences of that loss, if any. The real issue is not the loss of privacy, but abuse of personal information.
In my opinion, what we need to do is ensure non-discrimination and make certain that genomic information will only be used to improve any individual’s (medical) care. (The data can become part of studies, anonymized or not; we also need to redefine consent, but I am going to leave that out of this discussion too.) In other words, genomic information must only be used to enable and allow human beings to flourish.
Even a word like “flourish” or “thrive” is highly ambiguous, though. I mean it in a non-materialistic manner, whereas some others do not at all. Perhaps I can break it all down into stages to show what I mean within this specific context. Perhaps I can break it down to show what I mean within this context.
You mention the Hippocratic Oath, which some define as “Do no harm”. Harm is another concept that we don’t agree on yet and that we – therefore? – haven’t been able to define well.
I think that we need to start applying the principle of non-discrimination to all new human life. I believe that we should consider every human individual is just as valuable – in a non-materialistic manner – as every other human individual.
When I toss this around, I run into a peculiar dilemma. While I must see a deaf or a blind person (as an example) as equally valuable as a hearing or sighted person, I cannot accept it when a hearing or sighted person is deliberately made (permanently) deaf or blind, for instance during a mugging or a work-related accident. This also applies with regard to so-called augmentations. I cannot take a human being against his or her wishes and carry out a nose reconstruction or even inject botox. That makes me realize that harm done to a human appears to be any interference or change that occurs against that human being’s wishes and is implemented by someone else.
For now, I have to limit this to physical changes because the area of psychological changes is too complicated. (Just think of schools; we do not take bad teachers to court for being bad teachers, but we do take bad surgeons and physicians to court for being bad doctors, also because the evidence related to the latter is often much clearer.) Physical interference that occurs against a person’s wishes can of course also result in psychological changes, but that does not actually matter for the concept of harm within this context.
The next problem I then run into is the fact that particularly an embryo, fetus or newborn has a very limited ability to express wishes, but and that also holds for young children. If I try to put myself in the shoes of a child, however, it becomes possible to define harm in spite of that limitation.
This – putting themselves in the shoes of the child, as adults – is what parents, guardians and other carers do all the time, of course. They sometimes have to make the decisions for the child and express the child’s wishes for the child, as if they were the child, using the knowledge they have as adults, knowledge that the child will have in the future but does not possess yet.
So, lLet’s step into a child’s feet, then. It is hard to imagine a sick or injured child that would want to get sicker and sicker and sicker or want to have a permanently festering wound resulting from an injury caused by a fall. So it is fair to say that anything we do toward remedying such a situation is in accordance with the child’s wishes, in essence, even in cases in which the child cannot even say “please make the pain go away”. It is what the child would want if it possessed the knowledge and abilities of an adult.
So, the first step in part of enabling a human – a child – to flourish is to attempt to prevent any deterioration of the child’s health.
We may have to start agreeing that this cannot be considered harm within this context, even if the chance of success is small, certainly in cases for which there are no alternative remedies. We may even have to decide that doing nothing constitutes harm when there is still an option of doing something.
If a child has appendicitis, a surgeon will have to cut into the child’s abdomen in order to remove the appendix to prevent deterioration of the child’s health or even death. Strictly speaking, cutting into a child’s abdomen constitutes inflicting an injury, but in this case, as it is done with the intention of preventing greater harm, namely the deterioration of the child’s health, it does not constitute harm within this context we do not see it as harm. (This may be be an example of where I display a western bias?)
(Of course, we can still take the surgeon to court if his or her work fails to meet professional standards, but that is a different type of harm. We certainly need professional standards.)
We can also take a child to the dentist and the dentist may have to inflict some discomfort in order to prevent deterioration of the child’s health.
By contrast, we should not, however, drag a child along kicking and screaming to have its ears pierced as this is not done with the aim of preventing a deterioration of health. (If a child asks to have its ears pierced, there is a clear wish on the side of the child.)
Note that the intention matters. When a procedure is carried out with the intention of wanting to prevent deterioration of health, we never have 100% certainty that the intended result will be achieved. (This may have implications for how we think about practices carried out in other cultures. Keep this at the back of your mind. Our own western views are not the only views that hold value.)
The second step vital part of enabling a human being to flourish is to do everything we can within a daily-life context to allow that person to thrive on the basis of the person’s given physical (and mental) situation.
 We send children to playgrounds to let them play with other children and test their physical limits, we feed them, clothe them and provide shelter as well as love and all those other concepts that are hard to measure but easy to grasp. In essence, this is no different for children who are, say, blind or deaf or who have Down syndrome.
We send children to playgrounds to let them play with other children and test their physical limits, we feed them, clothe them and provide shelter as well as love and all those other concepts that are hard to measure but easy to grasp. In essence, this is no different for children who are, say, blind or deaf or who have Down syndrome.
The BBC news site just highlighted a very nice albeit exceptional example of what I mean by flourishing within this context: http://www.bbc.co.uk/news/m…
To do everything we can to allow that child to thrive is also required for children who are born with a medical condition that requires some form of medication or extra nutritional care to prevent deterioration of health. This, I think, is where standard genomic testing of newborns can play a pivotal role. These days, parents still too often have to conclude that something is seriously genetically wrong with their child on the basis of the deterioration of the child’s health, which in some cases means that irreversible damage has already occurred to the child’s health.
So, failure to provide such testing (screening) from the point in the future at which we know how to do and use this properly and reliably could perhaps also be seen as harm as it could lead to the preventable deterioration of a child’s health and would not encourage the child to thrive.
The third step next level within this context of enabling someone to flourish – and this is where it gets even trickier – is interfering with the child’s genetic make-up.
We may feel that the child is flawed, whereas the child is actually viable and does will not suffer a deterioration of health or be at great risk of certain complications if we allow it to live. At the moment, we often prevent such a child from coming into the world. This is where, I think, we need to draw the line and have to take a step back. It is a discriminatory practice because it appears to express a value judgement.
I also think that because of limited resources, we may need to approach this in a stepped manner.
What I mean is that if we initially limit techniques like CRISPR and gene therapy to all situations in which a resulting child would have “a life not worth living”, then we might have a fairly just and affordable way to start implementing CRISPR, gene therapy and anything else that may come along. Once we’ve done that, we can slowly start to take it forward, extend it to other conditions. The costs of such techniques will come down. and if we start with rare diseases that are currently incurable, we also limit the initial costs of implementation.
The loss of privacy may actually become an advantage because openness makes it also much easier to detect abuse of information and to safeguard against discrimination.
One of the reasons why I strongly believe that we need to start implementing non-discrimination for all new human life is the following. Once humans start interfacing with technology, other so-called impairments – which are currently often either biased opinions or restrictions imposed by society – cease to be impairments, taking away much of the motivation for “correcting” these individuals.
Moreover, not only do we – the human race as well as society – need diversity, we may have future needs for abilities of which we currently don’t realize that some people possess them. Those may well be people who are currently considered “impaired” or “flawed”. Junk DNA was once considered just that, too.
As I already indicated, we need a workable definition of what constitutes a life not worth living and once we have one (I may have found one, by the way, based on the principle of humanity), we may end up concluding that these are the primary cases in which we actually have a duty to interfere with the child’s genetic make-up.
So I agree with you that we have to exercise restraint, in spite of all the enormously exciting developments we currently see around us. Discrimination is not the only concern and neither are interpretation and costs. We don’t know all the possible consequences yet of the application of any of those new developments, even if we think we do.
We have made many decisions in the past without asking questions that now are so blatantly obvious in hindsight. Did nobody foresee that insecticides might also affect bees and birds and amphibians, to name just one example of a past mistake, albeit a highly significant one that now also affects human fertility?
We have another reason to take it slow, namely the fact that laws and regulations lag behind, evolve in response to arising situations in real life, and rarely anticipate on what may happen in the future. Legal professionals, too, tend to think conservatively and in a geographically limited manner. It’s probably the UN and WHO who should start taking the lead in this area, and guide us into the future. Do they need a push? Should we apply pressure?
Because perhaps more than anything else, we need to work toward reaching a global consensus (including legislation) on such important matters, irrespective of how challenging and impossible that may seem. It was also once completely unimaginable that we’d have humans land on the moon, so if we did that, then we can accomplish so much more than we think we can.
How do we approach the future?
In the science, health and environment section of thehindu.com, an article appeared under the heading “Do we understand the genome well enough to let Big Pharma jump into it?”.
I left the following brief reply.
You make important points.
Markus G. Seidel, who works at the Department of Pediatrics and Adolescent Medicine of Medical University Graz in Austria, just wrote something similar on the site of the BMJ, with regard to babies. He asks whether genome screening for newborns will pave the way to genetic discrimination. He too raises the question about interpretation (and reliability) of such data. He also discusses privacy issues.
But I wanted to write more…
 With regard to the latter, I think that humanity will slowly have to accept that the digital age comes with the loss of privacy in many ways. Privacy is a changing concept and there also is a cultural angle to it, so people from different generations and from different cultures have slightly different views on what privacy is. We probably should become more relaxed about the loss of privacy as we knew it and focus more on preventing and ameliorating potential negative consequences.
With regard to the latter, I think that humanity will slowly have to accept that the digital age comes with the loss of privacy in many ways. Privacy is a changing concept and there also is a cultural angle to it, so people from different generations and from different cultures have slightly different views on what privacy is. We probably should become more relaxed about the loss of privacy as we knew it and focus more on preventing and ameliorating potential negative consequences.
In my opinion, what we need to do is ensure non-discrimination and ensure that genomic information will only be used to improve any individual’s (medical) care. In other words, genomic information must only be used to enable and allow human beings to flourish. All human beings. In a non-materialistic way.
(Note that this is not the same as eradicating everything we may not like. But we seem to have a tendency to want to do that, unfortunately, and we need to curb that urge. We need a great deal of diversity to function well as a species and as a society, for many reasons. Good and bad cannot exist without each other – as cheesy as it may sound. There simply is too much we don’t know yet, and we therefore cannot foresee all possible consequences of everything we do. Eradicating everything that seems bad to us may be bad too.)
That will require two things: good legislation and regulations and a global consensus on these issues.
Particularly the latter is a major challenge. That is why we need to discuss these topics broadly and entice people to move out of their mental comfort zone, allowing them to explore other people’s views without instantly rejecting them. Our own views aren’t the only valid or even valuable views, but they tend to feel that way to us.
Legislation, however, also has a problem as it currently tends to display a big lag relative to what’s technologically possible. It does not anticipate (much), but responds after what is happening in practice forces it to respond. Also, legal scholars still tend to contemplate situations and consequences with regard to their own jurisdictions only.
So it looks like there is a great need for discussions pervaded by a spirit of tolerance (the willingness to step out of one’s mental comfort zone and listen to people from other cultures and generations) and a forward-thinking attitude.
By “forward-thinking”, I don’t mean “blindly embracing everything science and technology have to offer” because in the past, we’ve often forgotten to ask many questions we should have asked. That, for example, appears to have happened when we embraced pesticides. They seemed such a good thing, initially, that we never considered their obvious potential for bad.
Do you agree or do you see it differently? Do you think we also need to change big pharma, and if so, in which ways, and how could we approach that?
PS
I write from my own perspective of an opinionated white woman in the west without ties to big pharma.
Charlie Gard case – update
Playing God
There was a time when doctors were being accused of playing God when they helped patients stay alive. Now they’re accusing doctors of playing God when doctors don’t want to force a baby who isn’t viable to stay alive. (Alive?)
There is a lot wrong in the medical world. I agree. And I too have had to tell doctors things they didn’t know about although they’re supposed to be the experts and I admit that it used to surprise me. Discovering that I sometimes knew more than the doctors I went to for advice.
I don’t have the impression that the Charlie Gard case is one of those.
Charlie is being abused, by having been forced to stay alive this long. He is NOT fighting.
After having been forced him to stay alive – against nature – for so long, the decent option is now to let him have that experimental treatment, as I’ve said in a previous post.
But what will happen if the treatment has no effect? There will be more accusations, more lawsuits and more media drama because this stopped being about Charlie Gard a long time ago.
They will then fight to continue to keep him on a ventilator. (The disagreement in court yesterday about what one of the parents apparently had said three months ago seems to indicate that, along with the statement that the parents will continue to fight for the baby as long as he continues to be on a ventilator.)
That said, there are no 100% guarantees in medical matters. Sometimes, someone does wake from a coma twenty years or so later. True. But someone who ends up in a coma used to be viable. That makes a big difference. It means there was a well-functioning body with the healing abilities that entails.
“We will not be silenced,” they chanted.
Like I wrote above, this ceased to be about a little baby a long time ago. (I had that feeling from the beginning but I was not sure about it, and kept my opinion to myself until very recently.)
This is just as consumerist as wanting to design your own babies according to specs.
I hope that I am wrong about this. I do. I hope that they’ll take Charlie to the States and that a miracle occurs and he’ll grow into a strapping young man. But that’s not going to happen and I am afraid for little Charlie who is denied a say in this and who will also be denied a say if the treatment has no or no significant effect.
I heard a very significant mistake by an American news anchor yesterday. She talked about the current “treatment”. But Charlie Gard is not being “treated” and the legal proceedings are not about GOSH wanting to stop a treatment, which some people apparently seem to think.
Read this, too (GOSH statement):
https://t.co/X9WHHjhl3u
Read also this (opinion piece in The Guardian):
https://www.theguardian.com/commentisfree/2017/jul/09/the-guardian-view-on-charlie-gard-reason-and-unreason?CMP=soc_3156
Also, there are huge differences between Charlie Gard’s situation and the situation of Ashya King and his parents, as I have mentioned before.
See: https://www.judiciary.gov.uk/judgments/judgment-and-family-court-orders-in-the-matter-of-ashya-king/
Ashya King is healthy now.
Charlie Gard matter in court again
Is all of this still about Charlie Gard, actually?
Or is this an expression of a consumerist view of children?
Been wondering about that for a while now…
http://edition.cnn.com/2017/07/10/health/charlie-gard-new-hearing/index.html
The parents seem to claim that Charlie is “fighting”. But if he was, he wouldn’t require life support. He is being kept alive artificially.
Charlie “fighting” would be to take him off life support and finding him able to live on his own, surprising them all.
https://www.theguardian.com/uk-news/2017/jul/10/charlie-gard-key-questions-answered
It’s true, though, that if this child had been in the US, the experimental treatment would already have started and doctors would have a better idea of how it would affect the child.
With the case having been dragged through the courts for so long, and the postponements in terminating life support and allowing the child a peaceful passing, it’s now becoming more logical to allow the kid the treatment, if only because he’s been forced to stay alive so much longer now and would already have passed away if it hadn’t been for the legal battle.
If this news article is correct, though, then the parents’ battle is not about what is best for Charlie, by the sound of it:
http://www.wxyz.com/news/national/baby-charlie-gards-parents-storm-out-of-court-hearing
“Yates interrupted Francis as he said that the parents had said they would not want to prolong Charlie’s life in its present state, only if there was hope of improvement. “I never said that!” she exclaimed from her seat behind her barrister.”
Let’s see if I can find this back in Joshua Rozenberg’s tweets. Yes. Though he does not specify what the disagreement was about.
Chris Gard and Connie Yates storm out of court after disagreement with judge about what they had said during the hearing three months ago.
— Joshua Rozenberg (@JoshuaRozenberg) July 13, 2017
Nature itself considers Charlie Gard absolutely not viable. That is a very strong clue. Nature does its best to limit lives not worth living as much as possible.
Forcing Charlie Gard to stay alive is like insisting on having a purple parrot if its natural color is green and the other color goes with, say, severe liver disease. That’s not about what’s best for the parrot.
(I apologize to those who feel hurt by putting it this way. Maybe I should add that I had a green parrot for 21 years and loved her very dearly.)
How to deal with British police
Essentially, you don’t. You avoid them as much as you can because in Britain, you must consider police your enemy. They are not on your side. They are on their own side.
(Note: Anything I say on this page won’t stop me from, say, buying donuts for random police officers when they’ve all been called back from leave and are working very long days out on the streets. I do my best to see them as individual people.)
The only good reason for going to a police station in Britain is when you need to do that to be able to make an insurance claim.
Police in Britain stopped investigating crimes against individuals at least 10 years ago because they lack the resources to do so. The only crime against an individual that they are still bound to look into is when that individual has been murdered or if the individual is a supermarket owner or the like they like and someone has stolen a sandwich because he or she was hungry and was, say, caught red-handed or recorded on CCTV.
Other than that, forget it. That does not have to leave you stranded in all cases in which you’d normally expect to be able to get assistance from the police officers whose salaries you pay for through your council tax, after all.
Below are some tips, first for if you are a crime victim and second for if police are targeting you, for instance, because you are a crime victim.
Here is the GOLDEN RULE:
If police officers knock on your door, never ever open the door. Under no circumstances.
(You can still talk with them through the closed door, if you feel that it’s useful or required.)
1. Are you the victim of a crime?
Unless you need to do this for the sake of an insurance claim, do not go to the police. If you go to the police, the officers may tell you that they will use the information you give them as intelligence (though they won’t tell you that they are more likely to use it against you than against the perpetrator of the crime(s) you are reporting).
In almost all cases, they will also tell you to go to your council (civic offices) and to your GP. Don’t take it personally when they do this, even though it may sound like they are suggesting that you need mental health assistance. (After all, how on earth can a GP help solve a burglary, for instance?) They say this to just about everyone all over the country. It’s nothing personal; it‘s merely national policy.
You can investigate and try to stop crimes having been or being perpetrated against you but you have to proceed very carefully.
- What you need to do first of all is print several copies of the Protection from Harassment Act 1997. Tuck one away in each of your bags or suit pockets.
- Next, you write a letter to your local MP and any other politicians and/or journalists worth contacting. You explain to them what happened or is happening (the crime), in no more than one or two sentences, such as “My home was broken into” or “My daughter is being stalked. This has been going on for two years and last week the stalker broke into her home”. Then you write that you “will be approaching persons and taking actions for the purposes of preventing or detecting crime, pursuant to and in compliance with the Protection from Harassment Act 1997, Section 1, subsection 3, sub a.” and that you are sending this letter to him or her for his or her information. Send this letter or these letters by Special Delivery. Yes, that will cost you a few bucks but it’s worth it.
- If the MP or anyone else you wrote to then asks or tells you to go to the police, ask the person in question to come with you.
- Use Word or any other program to type up the following text: “Pursuant to and in compliance with the Protection from Harassment Act 1997, Section 1, subsection 3, sub a, I am approaching you for the purposes of preventing or detecting crime.”
- Print several copies of that text and always have them with you during your crime investigation. Before you say anything else, say this and hand the printout to anyone you want to speak with in relation to the crime in question.
- Also begin all your e-mails with that sentence if the e-mail is sent for the purposes of preventing or detecting crime.
- Remain reasonable at all times. That means, do not behave as if you are a police officer, do not get rude and do not lose your temper. You can certainly be firm. You are standing up for your rights. That is perfectly normal in many other countries and it’s a cry and shame that police in Britain don’t help you protect yours.
- Never undertake any of your crime investigation activities on your own, but always ensure that you have at least two witnesses, not from your family, but perhaps a colleague from work, a fellow member of a sports club you belong to or a neighbour or a client.
- If you do go to police, tell them as little as possible. They will use anything you report to them as “intelligence” and while they may inform you of that, what they won’t do is let you know that they may well use any information you give them against you. Police officers may act very friendly and reassuring, and talk about the action they will take, but when they do, they are usually just lying to you, unfortunately.
- The Protection from Harassment Act 1997, Section 1, subsection 3, sub b also means that it is very good (essential) to know the nature of the crime you are investigating, in legal terms. Look up which law applies to what happened, and why what someone did or does was or is a crime according to the law. You can go to the CAB or any other advice organisation, make some calls, see solicitors for a free half-hour consultation, drop in on a law clinic from your local law school and of course research it online and in books.
2. Are you being targeted by police?
British police officers these days seem to go after just about any person that they perceive as easy prey for their arrest (and prosecution) records and whose name and address they have. This could be someone who is probably poor or lower-class, someone who they suspect has a mental health problem and also someone who lives on his or her own or will likely only have kids in the house. So that there won’t be a partner who says “wait a minute!” and they only have to deal with one adult who police officers think will be intimated. Police officers know very well what effect they have on normal citizens and they exploit it when it serves them.
They also are more likely to go after people they don’t like, such as people who report serious crimes and are inexperienced enough to keep asking police officers what they are doing about it, particularly if the person lives on his or her own or will likely have only kids at home.
The problem with reporting a crime is that in the process, you give police officers a lot of information about yourself. They have your name and address now and know what you look like. By contrast, they very likely do not know the identity of the person who committed the crime or is committing the crimes you are reporting. They do now know also some of your personal circumstances, such as that you just broke off your relationship, got fired, just started a new job, whether you rent or own your home and things like that.
If you become the victim of a crime, no matter what cause of action you take (go to the police and/or investigate yourself), it raises the probability that police will start targeting you.
Under no circumstances report a crime and then keep calling to ask what the police officers are doing about it, even if a police officer has told you to do so. (Don’t investigate and report on your investigations either, not even if they have specifically asked you to do so.) All of this is bound to annoy them so much that you may well find them knocking on your door on Sunday morning at 7 am, when you innocently open the door and then find the door slammed into your face and yourself crushed onto the floor and arrested, your kids watching scared and helpless.
Unfortunately, that is the reality in Britain. It happened to Michael Doherty, for instance.
If you’re a woman, it may be more likely that police officers will call the local mental health hospital behind your back and suggest that you are mentally unwell. They may also pay your employer a visit and anyone else who suggesting to that you are not well in the head may disadvantage you.
That too is the reality of Britain today.
Do not open the door if police officers (are targeting you and) knock on your door. You do not have to open the door if police officers knock on your door, no matter what they tell you (with very few exceptions and in those cases, it makes no difference whether you open the door or not, so, don’t). That’s right.
Police officers can sound very convincing when they tell you all sorts of bullshit. Some of them are genuinely convinced that they know the law because they have this law book specifically for police in which they can look things up. If it says anything that does not suit them but would be to your advantage, they won’t tell you that. It will almost never come back to bite them anyway. In practice, police officers in Britain rarely have to adhere to the law, let alone administer it appropriately.
If you ever get arrested, don’t trust whoever shows up as duty solicitor either. He or she will not be interested in your rights. He or she will either want to get out of the police station as soon as possible or milk the circumstances for whatever reason. Of course, there are exceptions – GOOD and HONEST lawyers do exist; in fact, a few of your personal heroes may be lawyers – but under no circumstances assume that a duty solicitor will look out for you.
If you are investigating crime committed or being committed, someone may still call the police and say that you are harassing him or her. This is more likely if that person is the person who committed or has committed the crimes you are investigating, of course, because he or she knows that your powers are nowhere near those of police officers and may have more experience with police than you. He or she will want to make you go away and complaining about you is a possible approach to that.
That is particularly why you need to know what the Protection from Harassment Act 1997, Section 1, subsection 3, sub a says so that you can say that and maybe even show the printout of that law. Do not count on a duty solicitor to do that for you!
The fact that you are investigating crime on your own already indicates that you are not a person in power, after all. It makes you easily dismissible in the eyes of the police and in the eyes of the duty solicitor. Stand your ground. Don’t let them walk all over you. (You were doing what police officers should be doing. It is not your fault that, as a rule, they no longer deal with crimes committed against individuals these days.)
Also, you have informed several persons such as for example your MP about what you were going to do and you have witnesses.
Last but not least, a bit of a warning. Shana Grice, a young woman who reported being stalked to police was accused by police of wasting police time police (and fined, I believe) before her stalker killed her. There are other women in Britain who were killed by their stalkers, and they too were often not taken seriously by police.
I know a woman who was in similar circumstances, in the Netherlands. Her ex-boyfriend started stalking her and strangled her almost to death one day. In stark contrast to British police, Dutch police did not dismiss her but were very helpful. They advised her to relocate to a town in which she did not know anyone so that her ex was least likely to look for her there.
She took the advice, even though it meant breaking off her Master’s. She moved to a town at quite a distance from where she used to be and also from where her family was, enrolled in a lower-level educational program, then enrolled in another Master’s and after that started a PhD track. She got that PhD and she’s also a mother now.
(He eventually tracked her down in her new town too, but it took him a long time, and by then, he was less angry. One of her house mates or neighbors found him on the doorstep one day, and convinced him to go back and leave the woman alone.)
If you are being stalked in a way that seriously worries you, do not investigate or try to stop it by yourself (and certainly don’t bother reporting it to British police, also because they are likely to inform your stalker of everything you told police, whether on purpose of accidentally). Do what Dutch police advised this young Dutchwoman.
Hopefully, you’ll never need to know any of the above.
If you do use any of the above, and you end up killed, stabbed, bullied, hacked, arrested or anything else that you would have preferred to avoid, then note that you cannot hold me liable for any of that. I am not a lawyer, certainly not within this context, and I am not in a position to shield you from all risk.
Like the woman I mentioned above – no, it wasn’t me; it concerns a much younger woman whose acquaintance I made when she was working on her PhD – I too have only very positive experiences with Dutch police, even in sensitive circumstances that could have easily created friction and for which the officers in question had no training. Hats off!
I have worked with Dutch police in a neighbourhood crime prevention initiative. I also have positive experiences with American police, but race riots broke out in the US city where I used to live only shortly after I left. As we all know, American police has its troubles too because there had been too many incidents in which innocent black persons were killed by police officers in that city.
I think such incidents are often the result of irrational fears on the side of the police officers who often work under a lot of tension. I have personally witnessed in the US that when I had to call police in highly suspicious circumstances, they seemed much more scared and nervous than I was (presumably because I was living in a Florida neighbourhood that didn’t have a good reputation at the time). They were also looking out for my safety extremely well and I noticed that with gratitude.
I wish I could be more positive about British police.
I post the following from the work of Dr Lorraine Sheridan, as this can be vital information to have.
Typology 4: Sadistic stalking (12.9%)
Characteristics
· victim is an obsessive target of the offender, and who’s life is seen as quarry and prey (incremental orientation)
· victim selection criteria is primarily rooted in the victim being:(i) someone worthy of spoiling, i.e. someone who is perceived by the stalker at the commencement as being: – happy – ‘good’ – stable – content and
(ii) lacking in the victim’s perception any just rationale as to why she was targeted· initial low level acquaintance
· apparently benign initially but unlike infatuation harassment the means of intervention tend to have negative orientation designed to disconcert, unnerve, and ergo take power away from the victim
– notes left in victim’s locked car in order to unsettle target (cf. billet-doux of infatuated harassment)
– subtle evidence being left of having been in contact with the victim’s personal items e.g. rifled underwear drawer, re-ordering/removal of private papers, cigarette ends left in ash trays, toilet having been used etc.
– ‘helping’ mend victims car that stalker had previously disabled · thereafter progressive escalation of control over all aspects (i.e. social, historical, professional, financial, physical) of the victim’s life· offender gratification is rooted in the desire to extract evidence of the victim’s powerlessness with inverse implications for his power => sadism
· additional implication => self-perpetuating in desire to hone down relentlessly on individual victim(s)
· emotional coldness, deliberateness and psychopathy (cf. the heated nature of ex-partner harassment)
· tended to have a history of stalking behaviour and the controlling of others · stalker tended to broaden out targets to family and friends in a bid to isolate the victim and further enhance his control
· communications tended to be a blend of loving and threatening (not hate) designed to de-stabilise and confuse the victim
· threats were either overt (“We’re going to die together”) or subtle (delivery of dead roses)
· stalker could be highly dangerous– in particular with psychological violence geared to the controlling of the victim with fear, loss of privacy and the curtailment of her social world
· physical violence was also entirely possible
– especially by means which undermine the victim’s confidence in matters normally taken for granted e.g. disabling brake cables, disarming safety equipment, cutting power off
· sexual content of communications was aimed primarily to intimidate through the victim’s humiliation, disgust and general undermining of self-esteem
· the older the offender, the more likely he would have enacted sadistic stalking before and would not be likely to offend after 40 years of age if not engaged in such stalking before
· victim was likely to be re-visited after a seeming hiatusCase management implications
· should be taken very seriously
· acknowledge from outset that the stalker activity will be very difficult to eradicate
· acknowledge that there is no point whatsoever in appealing to the offender – indeed will exacerbate the problem
· never believe any assurances, alternative versions of events etc. which are given by the offender
· however, record them for use in legal action later
· the victim should be given as much understanding and support as can be made available
· the victim should not be given false or unrealistic assurance or guarantees that s/he will be protected
· the victim should carefully consider relocation. Geographical emphasis being less on distance per se, and more on where the offender is least able to find the victim
· the police should have in mind that the sadistic stalker will be likely to:(i) carefully construct and calculate their activity to simultaneously minimise the risk of intervention by authorities while retaining maximum impact on victim,
(ii) be almost impervious to intervention since the overcoming of obstacles provides
(iii) new and potent means of demonstrating the victim’s powerlessness (ergo self-perpetuating) and,
(iiii) if jailed will continue both personally and vicariously with the use of a network.
http://www.le.ac.uk/press/ebulletin/archive/speaker_sheridan.html
http://www.le.ac.uk/ebulletin-archive/ebulletin/features/2000-2009/2007/07/nparticle.2007-07-17.html
The courts and the Charlie Gard case
I’ve noticed that several people landed on my site because they were looking for an update in the Charlie Gard case. Well, the European Court has declined the case as well.
It occurred to me that if you want to learn more about how courts arrive at the decisions they make, then this book can be a good start.
Northern Ireland abortion refugees: Supreme Court — UK Human Rights Blog

R (o.t.a A and B) v. Department of Health [2017] UKSC 41, 14 June 2017 – judgment here. Sometimes The Law comes to the rescue. And by this I do not mean constitutional law versus populism or the rule of law versus raw-knuckled fighting. It just happens that, occasionally, litigation drawn from ordinary life encapsulates more political […]
via Northern Ireland abortion refugees: Supreme Court — UK Human Rights Blog
Human rights for just a few, that’s discrimination. Human rights apply to all human beings.

It has just been the 6th anniversary of an important human rights case, that of Mark and Steven Neary. Steven, who is autistic, was detained in local authority care for over a year before his dad used the Human Rights Act to get him home. RightsInfo has made a powerful short film to mark the […]
Abortion
Writing the first version of my essay “We need to talk about this” – the updated is in the works – forced me to think about issues I had never thought about before in great depth and I had to leave many of them untouched at the time.
For example, I am a feminist and I have always believed in a woman’s right to abortion. While I was considering how we could regulate the new eugenics, I ran into boundaries. It included having to think about how to fit abortion into the topic. That was a significant hurdle.
I was no longer able to say “of course women should be able to have abortions” – which I had always done in the past – but had to think about why and when they should, regardless of my own personal feelings. Because what I was writing about selecting pre-embryos and fetuses clashed with the general ideas that I had always entertained about abortion but had never examined in detail.
Legislation and protocols can sound very cold to people, but it’s not enough to just state something like “we think this is very very good” or “we think this is very bad”. That wouldn’t work in practice. If you want to make sure legislation is solid and leaves little room for abuse (deliberate misinterpretation), you end up with language that can come across as heartless. But that does not mean that the legislation (or protocol) is heartless or that the people who wrote it are!
It can be difficult to get that across, I have seen in various online comments (on for example the Groningen Protocol). It works the same way for traffic rules or rules for building skyscrapers. The law can’t just say something vague like “drivers should be careful” and “buildings should be safe” and leave it at that.
When Obamacare was introduced, a staunch Republican (and stauncher Libertarian) wrote to me that it was ridiculous that its legislation was taking up more than 2,000 pages or something like that. (Who would ever read that?)
I replied to him that I knew a jurist who works in precisely that area in the Netherlands and explained what that kind of legislation has to include. Fortunately, he listened to that explanation.
Unfortunately, I have found that even people who see themselves as the voice of reason (and sometimes as having absolute wisdom, too) aren’t always willing to listen to what someone “from the other side” is saying.
A certain brand of callousness
In my essay “We need to talk about this” I mention that I have on occasion been shocked by a certain brand of callousness that I have seen (too) often in Britain (both in the media and in real life). Here is one example of what I mean.

You can only justify such occurrences by applying a tweaked form of utilitarian reasoning. One person was suffering, but “wasn’t really harmed” and the number of people who were enjoying what was being done to George Cheese was greater than 1, hence these occurrences “increased overall happiness”.
The fact that utilitarianism was associated with the higher classes may have given this type of reasoning or events an unfortunate aura of “cleverness”. It could also explain why anyone who condemns the sort of things that were being done to George Cheese is seen by some as “naïve” and “not quite with it”.
Utilitarianism also attached little importance to individual persons’ rights. It would have stopped short from, say, stabbing someone like George Cheese as opposed to setting his clothes on fire and stuffing him into the trunk/boot of a car. This is the kind of background, I think, that enabled Simon Wright to say “It did not go too far.”
In reality, abuse targets like George don’t get to LIVE. All they are allowed to do is wait for their natural deaths. George Cheese said “FUCK THAT!” and stood up for himself in the only way he had left.
At least there is an inquest. That’s good.
The Charlie Gard case
Ouch.
I ran into the story a while ago, and couldn’t find too much information about it back then. However, the parents have just been turned down by the next court and now apparently plan to take the case to the Supreme Court. That’s resulted in more attention for the story, with more background.
Here are two places where you can read more about the case if you’re not familiar with it:
http://www.bbc.co.uk/news/uk-england-london-40047485
https://researchingreform.net/2017/04/12/london-live-interviews-researching-reform-on-charlie-gard/
http://www.bailii.org/cgi-bin/format.cgi?doc=/ew/cases/EWHC/Fam/2017/972.html
In the online discussions, I see something that I also recently mentioned in an essay I wrote and I feel the need to say something about that. (I have also submitted a comment elsewhere.)
Yes, it is true that the British medical profession can be extremely arrogant. As a Dutchwoman who previously lived in the US and is now based in Britain (in Ashya King’s city, I might add), I too feel that the medical profession generally still has that ridiculously old-fashioned god status in Britain. I’ve for instance been ridiculed by an ophthalmologist for asking about possible side effects of a medication, only to find that it did cause serious problems for me. (Thankfully, we have the internet now, which can help us solve such relatively minor problems and bypass physicians who don’t like assisting emancipated patients.) Some people have mentioned Ashya King’s case within this context.
Having said that, Charlie Gard’s case – heart-breaking and difficult – also has a strong element of the opposite. We are now in an era in which doctors are increasingly often perceived as “playing God” when they do NOT do everything in their power to prolong a baby or an adult’s life artificially, no matter how high the cost to the individual in question.
Charlie Gard’s case is not comparable with Ashya King’s case.
Charlie was born with a condition that normally means the infant won’t live very long. I understand that of the few children with his condition, his situation is the worst. Ouch. One can ask whom prolonging Charlie’s life benefits, Charlie or his parents. This will sound incredibly harsh to many and I understand that. It is okay to be very angry with me for that comment.
(I understand, really. I grew up with illnesses and deaths in my very close surroundings; it concerned my mother, one of her sisters and one of her brothers. They died of different kinds of cancer. My mother suffered greatly and for many years, after having been misdiagnosed twice. My youngest sister almost died after she was misdiagnosed when she was 4 or 5. She ended up in critical condition and had to be cooled with ice to keep her fever alone from killing her.) If it hadn’t been for the persistence of my dad, she would never have had the chance to develop into the successful business owner she is today. So, yes, I do know about losing people and wanting to hold on to them.)
On the other hand, allowing Charlie the experimental treatment in the US could yield very important information that may not benefit Charlie but could benefit future infants with mitochondrial DNA depletion syndrome or even other conditions. Could that be worth it? Hard to say.
What would Charlie want? Can you place yourself in Charlie’s situation for even a moment?
Ashya King, by contrast, was a healthy and much older kid who developed a brain tumor. Even with the traditional treatment, Ashya had a fighting chance and treating Ashya as well as possible was certainly going to benefit Ashya (even though there is never a 100% guarantee).
And it has.
One of our problems is that we badly need global regulations for all kinds of medical situations, regulations that people from all sorts of backgrounds all over the world can agree with. The lack of it currently not only causes medical tourism but also the kind of heartbreak we now see in the Charlie Gard case.
If I put myself in the parents’ shoes, I say that most of the hurt and upset for them is currently coming from the legal process. The uncertainty. Even possibly the knowledge that every day they spend in court is one day on which he is not getting the experimental treatment in the US. Unassisted, nature would have already allowed Charlie to cross the rainbow bridge and be at peace and the parents could have had a more normal mourning process.
Is Charlie at peace now? Is he not? How can we know?
It might be possible to avoid this kind of agony if we had much more clarity about what to do to limit harm to such a child as much as possible. Such regulations will have to be a compromise, obviously, and can never avoid heartbreak (but heartbreak is also a normal part of life; life does not come with guarantees and the losses make us cherish what we have).
Conditions like Charlie Gard’s also play a role in the new eugenics, currently particularly in the selection of embryos for IVF procedures, a rapidly growing practice, and soon in the creation of designer babies. It is an incredibly difficult topic that is screaming for attention. So I just wrote a rather provocative essay on it, in a hurry. It is called “We need to talk about this” (the second edition is already in the works) and includes a definition of what constitutes a life not worth living. I have based it on the principle of humanity, namely that every human being has the right to a life in dignity. During the writing of that essay, I grew very depressed a few times, because it is such a hard and dark topic. But we really do need to talk about this, sooner rather than later.
I wish the judges and the parents wisdom and strength and little Charlie lots of eternal sunshine of every possible kind.

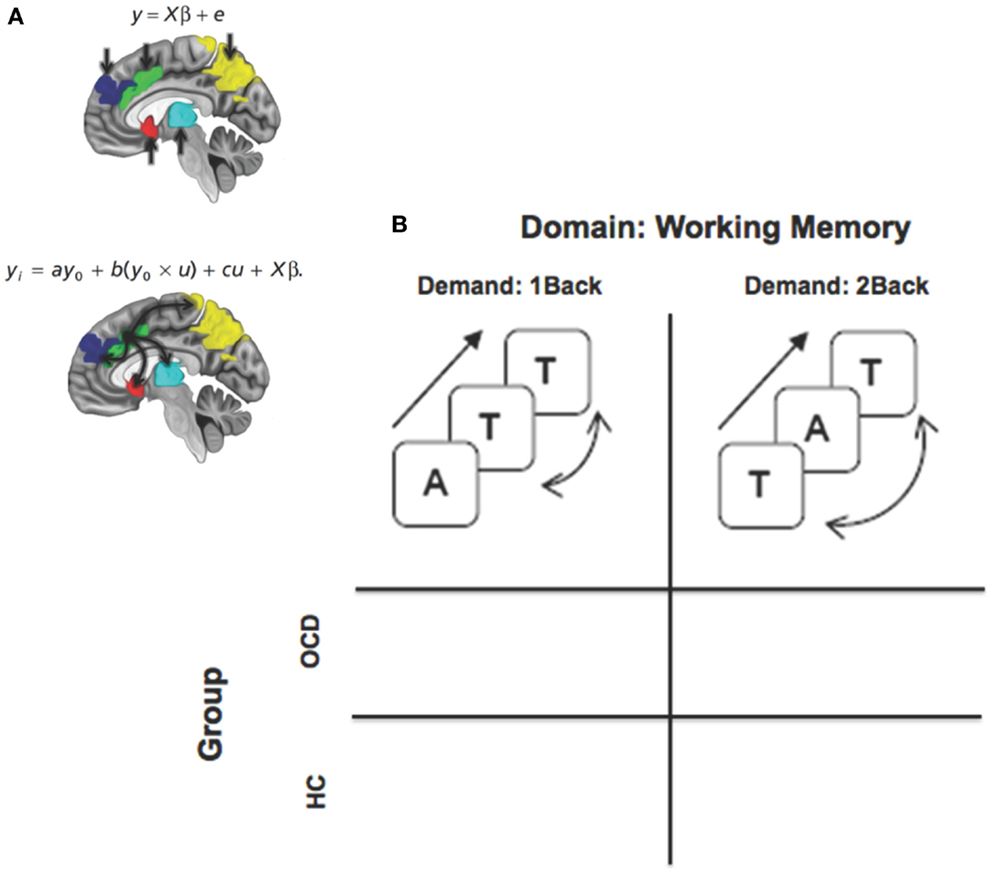{kind=link}